Our solution takes you from single cell or single-nuclei suspension through library prep and sequencing and delivers immediate results via our analysis software, Trailmaker.
Our solution takes you from single cell or single-nuclei suspension through library prep and sequencing and delivers immediate results via our analysis software, Trailmaker.
BLOG › Customer Profiles › Using scRNA-Seq to Analyze the Effects of Lung Inflammation in SARS-Cov-2 Patients
Using scRNA-Seq to Analyze the Effects of Lung Inflammation in SARS-Cov-2 Patients
March 29, 2023
|
14 min read
Updated:May 24, 2024
Imagine that as a young scientist you saw a formerly fatal illness become treatable. Now, imagine that major contributors to this groundbreaking result become your mentors.
It happened to Dr. Alejandro Pezzulo, MD, an Assistant Professor of Internal and Pulmonary Medicine at the University of Iowa. After witnessing the successful treatment of cystic fibrosis in 90% of the patients, he was inspired by the knowledge acquired from his mentors to tackle other deadly pulmonary diseases. Today he is on the frontlines to study and treat the effects of chronic lung inflammation in patients’ response to viral infection.
His work is more relevant than ever, as chronic lung inflammation is a risk factor for severe COVID-19 infection.
But what is chronic inflammation and why does it affect the way the body responds to pathogens? Inflammation is part of the body’s innate immunological defense against microorganisms, irritants, or damaged cells. Type 2 inflammation is a chronic type of inflammation, characterized by the release of cytokines such as IL-4, IL-5, and IL-13. It is commonly associated with chronic conditions such as allergies, asthma, and autoimmune diseases. Over time this leads to tissue damage, chronic disease, and ultimately to a weakened and compromised immune system, unable to effectively fight off infections.1
We sat down with Dr. Pezzulo to discuss his research on chronic airway type 2 inflammation in the lungs and its effect on patients’ response to COVID-19.
Dr. Pezzulo, you published a wealth of peer-reviewed research on cystic fibrosis, but more recently, you also studied infectious diseases affecting the airways. What fascinated you about cystic fibrosis and why the expansion to other areas?
There is an interesting story behind that. I work at the University of Iowa, home to a prominent group of physician-scientists and researchers studying cystic fibrosis.
My primary mentor, Dr. Joseph Zabner, is at the forefront of research to develop gene therapy for lung diseases.
Another of my mentors, Dr. Michael Welsh, has been studying this disease since before the sequence of the CFTR gene was published. He discovered the function of CFTR, and developed assays and cell models that enabled the pharma industry to eventually develop groundbreaking treatments.
In the last 3 to 4 years, the care of people with cystic fibrosis has changed dramatically, and today patients are doing amazingly better in part due to the research of my mentors.
As a young researcher and a trainee, it has been astonishing and inspiring to see what happens to patients, clinical operations related to cystic fibrosis, and related research fields once the disease is nearly cured.
I wanted to apply the knowledge gained to other areas.
Today I focus on the airway epithelium – the lining of cells in the lungs and airways. The epithelium protects us from bacteria, viruses, and particles we inhale daily. It also has other essential functions that allow our lungs to work properly. I want to understand how airway epithelium’s responses to the environment determine human disease.
Initially, I was interested in the epithelium interaction with bacteria. And cystic fibrosis was a great model because many manifestations of cystic fibrosis derive from a defect in how the epithelium kills bacteria.
Eventually, I became interested in understanding how and whether dysregulated inflammatory responses in the airways may result in chronic lung diseases like asthma and chronic obstructive pulmonary disease (COPD).
Can you describe how IL-13 became the focus of your COVID-19 research?
Before studying COVID-19, I researched how a process like goblet cell metaplasia caused by IL-13 affects airway and epithelial biology and how we can control it in asthma.2 For example, over half of asthmatic patients have excessive IL-13 activity in their airways, which has consequences including excess lung mucus.
When asthmatics get a virus infection, their lung function worsens, and often they are admitted to the hospital or the intensive care unit.
I started studying this phenomenon, and I was deciding which virus to study. Then the COVID-19 pandemic began and it chose the virus for me.
From a fundamental biology standpoint, I was interested in how different states of inflammation in the lungs affect our response to viruses. Coronaviruses, in general, have been around for a long time and frequently cause disease, even outside of SARS-CoV-2.
I wanted to understand if type 2 inflammation causes an excessive inflammatory response to the virus or impairs the response, making us more susceptible to excessive viral replication in the airways.
From a clinical standpoint, I work in the ideal environment to tackle this question. I care for people with various diseases in the intensive care unit, including asthma and virus-induced diseases. Early in the pandemic, we were not sure how asthmatics would do, and we were very concerned, as asthmatics tend to respond poorly when exposed to viruses.
This led us to the specific question: how does IL-13-induced inflammation affect the epithelial response to the virus and the overall host response to the virus?
Can you describe your experimental approach to answer this question?
Asthmatic patients have excessive inflammation. We decided to use exposure to IL-13 as a model of what happens in asthmatics.
Capturing these patients is feasible for me, as I run a research core in our institution that obtains and distributes human airway epithelial cells from patients’ lungs.
These cells are primary: they are studied as obtained from the lungs, without being turned into an immortalized cell line, as commonly used in research. We cultured them in vitro at the air-liquid interface, allowing them to differentiate into the same cell types they would have in vivo in a human to closely imitate what happens inside a human lung.
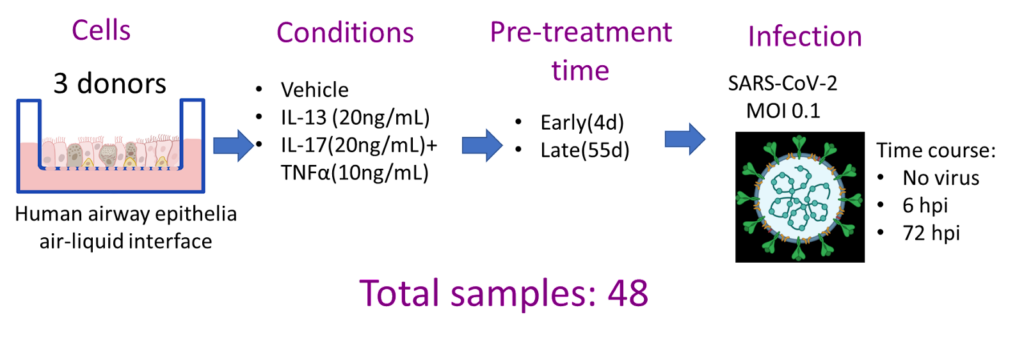
We cultured multiple cell samples from human lungs in this model, and exposed them to either IL-13 or IL-17 and TNF alpha, which are increased in other types of inflammation (Fig 1).
After exposure to these cytokines, we asked:
What will happen if we infect them with SARS-CoV-2?
Will they be more or less likely to be infected?
And if infected, will they respond differently whether they have had IL-13 or IL-17 and TNF exposure?
How will that affect viral replication and viral titer?
Fig 1:Study design: airway epithelial cells from 3 patients were cultured with different cytokines, infected with SARS-Cov-2 virus, and then tested at 6 and 72 hours post infection. Image courtesy of Dr. Pezzulo.
Before we talk about the results, can you touch on the importance of biological replicates in your experimental design?
This is an essential point because to extrapolate findings from our experiments to a broader population, in this case, other humans, we need to understand how the mechanism under study varies across different human samples, which we call a biological replicate.
Before Parse Biosciences’ technology became available, it took a lot of work to study replicates, primarily because of the cost of experiments using other technologies.
We chose Parse because it allowed us to study more samples in one experiment. This scalability made our investigation rigorous and interpretable, more robust in the long term.
In a single experiment, we were able to study the effects of both IL-13 versus TNF alpha and IL-17 on the response to the virus in short-term versus long-term cytokine treatment. We were also able to capture different time points after the infection.
By enabling us to run 48 samples in one experiment, we produced biological replicates, time points, and different interventions. We generated a large dataset that we are still analyzing from various points of view.
Can you describe what scRNA-seq data revealed in the 48 samples before and after exposure?
I want to mention that these results have not been peer-reviewed yet. What I am about to talk about is the same data I present at webinars.
Existing peer-reviewed research already showed that IL-13 seems to decrease ACE2 levels in vitro.3 But how and why was not clear.
Single cell sequencing showed us that the number of cells expressing ACE2 decreased after IL-13 exposure in the epithelium. However, the level of ACE2 expression in each cell was not regulated by IL-13. This observation is important to keep in mind when we interpret how IL-13 affects the susceptibility of the epithelium to the virus.
Does IL-13 affect the number of infected cells? Yes, it absolutely does. By running a time course experiment on 48 samples at the same time, we observed that the major effect of IL-13 occurred later in the exposure.
Following IL-13 exposure, cells underwent a process called epithelial remodeling – structural changes occurring in the tissue surrounding the airways in response to injury. There were changes in cellular composition: more mucus-secreting cells (goblet cells) and less ciliated cells, a condition that in vivo indicates chronic airway inflammation.
In this inflammatory context we found that IL-13 drastically decreased the number of cells infected with the SARS-CoV-2 virus, leading us to believe that IL-13 does reduce the risk of infection in all cell types.
The next question was whether IL-13 affects viral replication in cells infected by the virus. Single cell data showed that IL-13 does not affect viral replication within each cell, but still decreases the viral titers in the samples overall. This observation seems to suggest that IL-13 protects from the virus: while SARS-CoV-2 virus would enter the epithelia in normal conditions, IL-13-driven inflammation seems to block its binding and entry in the tissue.
However, further data, such as in vivo studies that are now underway, and randomized clinical trials are needed before we can change the current COVID-19 management practice.
What was your data analysis strategy?
Initially, we worked with the Parse bioinformaticians, using Parse’s pipeline for initial quality control, base calls, and alignment.
Then, we needed to analyze multiple replicates in one experiment. Until then, most published research compared condition A versus B without accounting for subject-to-subject variability.
But in this study, we have to account for biological replication, so the sample size has to reflect the number of replicates, not the number of cells within each sample as is commonly done.
How to account for both the multiple cells in each sample and the biological replicates?
When we were asking this question, the statistical approaches addressing it were just being developed.
Fortunately one of my lab members, statistician Andrew Thurman, reviewed the literature and tested different approaches to analyzing the data. We have a publication where we developed a straightforward method to analyze the data called pseudo-bulking that allowed us to optimize the false positive and the false negative rate in our analysis.4
Each sample may have thousands of cells, and there may be hundreds or thousands of cells for each cell type. But to analyze the data in a manner more closely reflecting or accounting for biological variation, we turned all the cells belonging to a cell type within a biological replicate into what we call a “pseudo-bulk” sample.
We then analyzed that data using tools that have been around for many years for bulk RNA sequencing, and that facilitated our initial analysis.
Since then, we have developed more elaborate and complex data analysis methods. But this was what we came up with back then.
What aspect of the Parse technology helped you overcome some of the biosafety obstacles of working with a potentially deadly virus?
A couple of aspects are critical. First, I want to thank Charlie Roco. I started working with him right before the pandemic or around when the pandemic was starting and Parse Biosciences was still called SplitBio.
In our initial discussions, I mentioned that it was intelligent of them to consider asynchronous samples in the protocol. The other methods at that point required having almost all samples ready simultaneously to start a scRNA-seq experiment since they require live cells already in suspension and ready to go.
One key aspect of Parse’s protocol that made our experiment possible is that by design, the protocol asks to fix the cells and to cryopreserve them. And this allows the user to work more consistently with standard research needs, especially involving human samples, as they usually come at different times. The user needs a protocol to process samples asynchronously to include multiple replicates. That was one key aspect of Parse that enabled us to do just that.
The second aspect is that during this process, Parse’s fixation method inactivates SARS-CoV-2. We worked with Charlie and the rest of the Parse team to do experiments on our end, and we proved that the fixation inactivated SARS-CoV-2.
When we showed these results to the biosafety committee of the BSL-3 facility, they gave us permission, upon sample fixation and freezing, to take them out of BSL-3 to the lab and finish the experiment there.
This was a logistical advantage that I don’t think we could have done without this aspect of the Parse protocol. Otherwise, the alternative is to bring a lot of equipment into BSL-3 that you can never take out of BSL-3, and then we don’t necessarily want to have it in BSL-3 only. This was a key aspect.
Let’s talk about your single cell experience. What advice would you give to other researchers pursuing single cell research?
I think about three main points that I can make.
First, have a hypothesis. These advanced technologies are becoming less expensive and can be applied to many experiments. It is helpful to go back to trying to have a good hypothesis before starting an experiment.
In other words, one can always do single cell biology under many conditions and ask broad questions to understand the system. However, having a specific hypothesis from the start is critical because it allows for deciding the sample size, the time points needed, and the concentrations of the interventions to use. Without that, one ends up with experiments that can describe many things but do not necessarily address a clear and specific hypothesis.
Second: have a good analysis plan. Involve the biostatisticians before the experiment starts while still formulating the hypothesis and the experimental design.
The third point is more practical and involves sample prep. In single cell biology, samples can be prepared in different ways. The single cell suspension preparation will differ depending on the cell type or the sample size. It is crucial to understand how well the cells can withstand the process to avoid issues like having a good single cell suspension but no viable cells in it.
Depending on the sample type, it takes some effort to set up a proven protocol, but once settled, the experiment can start. That is one way to avoid frustration for researchers.
Looking toward the future, what are your thoughts on the future of single cell research and genomics?
The basic unit of biology is the cell. Single cell biology will be the default, and it’s already becoming the standard.
I have been very excited about the role Parse has been playing in the single-cell biology arena, because I think that their scientists design things with adaptability and with good experimental design in mind. And in a way that most researchers can adopt the methods without using the whole year budget for just one experiment. Parse allows you to do things in single cell mode in general.
I’ve also found it interesting to see how different competitors in the same space have been reacting to how Parse has been doing things. And this speaks very highly about how Parse works.
The field is also going toward spatial biology. And besides transcriptomic analysis, there will be tremendous growth also in epigenetic assays, DNA, and other sequencing types of analysis.
What are you working on right now?
Related to this project, we are doing much work in vivo using novel models our group has developed to study coronavirus biology in mice. And we are currently doing our experiments on the same question in vivo.
And what's your next single cell experiment going to be?
We have been talking with the team at Parse for the past few days about an experiment where we tested the role of inflammation in the lungs in response to SARS-CoV-2 in vivo in mice.
Dr. Alejandro Pezzulo and his lab at the University of Iowa. From the left, front row: Grant Stalker, Shreya Ghimire, Lorena Tran, Huiyu Gong. Back row: Olivia Marshall, Andrew Thurman, Alejandro Pezzulo, Brandon Bettis, Grace Necker
Thank you, Dr. Pezzulo, for this fascinating conversation. If you want to learn more about this research, and how Parse Evercode kits facilitated Dr. Pezzulo’s work, watch this webinar!
References:
Rouse, B., Sehrawat, S. Immunity and immunopathology to viruses: what decides the outcome?. Nat Rev Immunol 10, 514–526 (2010). doi: 10.1038/nri2802
Pezzulo AA., Tudas, RA., Stewart CG., et al. HSP90 inhibitor geldanamycin reverts IL-13- and IL-17-induced airway goblet cell metaplasia. J. Clin Invest (2019) 129(2). doi: 10.1172/JCI123524
Jackson DJ, Busse WW, Bacharier LB, et al. Association of respiratory allergy, asthma, and expression of the SARS-CoV-2 receptor ACE2. J Allergy Clin Immunol. (2020) 146. doi: 10.1016/j.jaci.2020.04.009
Thurman AL, Ratcliff JA, Chimenti MS, Pezzulo AA, Differential gene expression analysis for multi-subject single-cell RNA-sequencing studies with aggregateBioVar, Bioinformatics, Volume 37, Issue 19, 1 October 2021, doi: 10.1093/bioinformatics/btab337